
From whichever angle one approaches the Covid crisis in India, it is clear that the Bharatiya Janata Party (BJP) led government is responsible for a catastrophic situation. In early February, the Health Ministry boasted that Covid had been defeated in the country. By the middle of April, the official cumulative tally for Covid positive cases was at 13.4 million, and the death toll was at a staggering 174,308. Both figures are now substantially worse.
On April 16, Adar Poonawalla, owner of the Serum Institute of India (SII), appealed to the Biden administration to lift the embargo on vaccine-related raw materials so as to fast-track vaccine production. In the gap between medicine and death, the CEO of arguably the largest vaccine manufacturer in the world stepped in as the savior, appealing for vaccine security for developing countries.
 As the largest vaccine manufacturer (by doses produced and sold) in the world, SII was invited early on (April 2020) as a scale-up partner to the consortium led by the venture capital-backed spin-out company Vaccitech Ltd., which developed the Oxford-AstraZeneca vaccine. Over the next few months, even as the consortium expanded and AstraZeneca won exclusive license rights to produce the vaccine, a great extent of its commitment to “make [the vaccine] available and accessible for low- and medium-income countries” relied on its sub-licensee SII.
As the largest vaccine manufacturer (by doses produced and sold) in the world, SII was invited early on (April 2020) as a scale-up partner to the consortium led by the venture capital-backed spin-out company Vaccitech Ltd., which developed the Oxford-AstraZeneca vaccine. Over the next few months, even as the consortium expanded and AstraZeneca won exclusive license rights to produce the vaccine, a great extent of its commitment to “make [the vaccine] available and accessible for low- and medium-income countries” relied on its sub-licensee SII.
Mr. Poonawalla’s demand placed him at the heart of several heroic imaginations. In the nationalist chronicling, here was the darling of the Indian nouveau elite, a person often called the “vaccine prince” of India, fighting valiantly to ensure that not only his nation, but all the poor of the developing world, had access to a life-giving vaccine. In the cosmology of the global commentariat, his tweet once again emphasized the importance of raw materials, intellectual property rights, technological knowhow, and international standards as barriers to be overcome if nations are to achieve vaccine security and biological immunity for their people. And in the subconscious of some sections of what might be broadly construed as the Left, he reignited the old dualities of the core and the periphery – the Cold War opposition between Global South and Global North – the imperialism of the West with Big Pharma on the one side, and the Third World on the other.
The TRIPs waiver and easing of global trade regulations has now become the rallying cry for citizens’ groups, NGOs, and social movements across the world. In their call for action, prominent economists like Joseph Stiglitz, Jayati Ghosh, Rohinton Medhora, and others have argued for greater funding and political support for COVAX and a short-term TRIPs waiver, along with debt restructuring, as central planks to minimize the disparities between the Global South and North. It is worrisome that the thrust of this politics in the name of vaccine imperialism continues to remain within the Cold War paradigm of the Global South versus the Global North.
Adar Poonawalla is the world’s 165th richest man, a person who, on the side, oversees a multimillion-dollar horse racing enterprise. The SII is nominally in the “Global South”; its CEO is among the class of global elite who have stellar resources, private jets, batmobiles, and residences in London, placing them in a world of luxury that is decoupled from the death and devastation unfolding around them. In an insidious inversion, the perpetrators of a vaccine famine have presented themselves as the strident defenders of vaccine sovereignty. Disaster capitalism is intimately linked to the organizational growth of fascism in the Indian context, starting at least since the late 1990s. The media may very well accord him the mantle of being the humanitarian who will give the Global South a fighting chance to defeat the virus. Remaining delimited by the framework of the Global North-South duality, however, obscures the two main battlegrounds on which anti-capitalist politics ought to be fought: the international economic governance structures around commodity flows in which the Indian state and capitalists like Adar Poonawalla are players; and the nexus between fascism and pandemic capitalism. How can social movements take on the Poonawallas, who, as we shall see, represents the brutal mercenary calculus of pandemic capitalism?
SII and India’s Vaccine Manufacturing Landscape
A full understanding of the complex international capitalist structures within which the SII fits first necessitates understanding its location within India’s vaccine manufacturing landscape, which we explore in this section.
After its consolidation as a nation-state, India’s successful Smallpox Eradication Program in the 1960s created a national health infrastructure with trained vaccinators, storage facilities, and a network for health monitoring that took it down the path to vaccine self-sufficiency. Between 1962 and 1971, nearly 19 public sector and 12 private sector vaccine manufacturing units were established. Initially strong in the urban areas, under the aegis of the Polio Vaccination Program (1985-1991), this infrastructure deepened its coverage across both the rural and urban sectors. Almost all Indian vaccine manufacturers today, like the Haffkine Institute (1895), Biological E Ltd. (1953) and Serum Institute of India Ltd. (1966) – but, notably, not Bharat Biotech (1996) – emerged during the early phases of the industry, though their fortunes now look very different.
With the onset of liberalization in the 1990s, the responsibility to develop and manufacture vaccines was gradually relinquished as the state created a conducive environment for domestic pharmaceutical companies like Ranbaxy and Cipla through Patents Acts, foreign investment regulations, and amended industrial policies. India emerged as a leading generic drug maker and vaccine supplier during this period and by the middle of the decade pharmaceutical firms had started consolidating through mergers and acquisitions.
In 1994, armed with a WHO accreditation, SII began to export its vaccines, thus placing it within global distributive networks via contracts with U.N. agencies. By 1998 SII was exporting vaccines to over 100 countries and in 2012, Cyrus Poonawalla acquired the Netherland-based vaccine maker Bilthoven Biologicals and the Czech arm of US-based Nanotherapeutics that opened up European markets for his company. Exports now contribute about 85% of the company revenues. Several factors thus came together to create the conditions that facilitated the near capture of the market by the SII: the mergers, acquisitions, and decline of public funding in the post-liberalization era that made the vaccine market more conducive to oligopolistic control; and the vast volumes of speculative capital from horse racing made it possible for the Poonawalla family to invest money in this market.
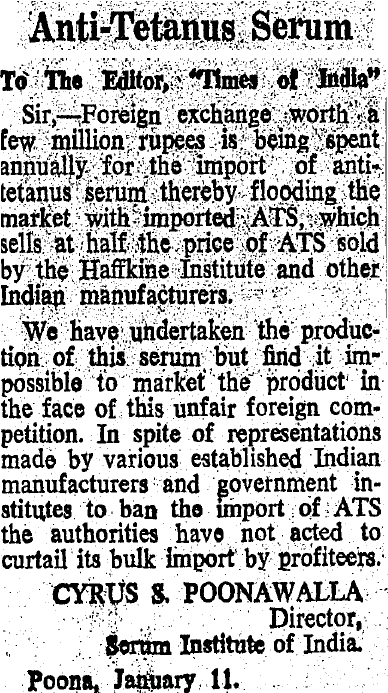
Growing out of a stud farm run by family patriarch and horse breeder-turned billionaire Cyrus Poonawalla in Pune, the Serum Institute thus had an unlikely origin for what would ultimately become a vaccine behemoth. The Poonawallas had been an old name in the horse racing circuits of India. Instead of retiring his racehorses to a quiet pasture, Cyrus Poonawalla put them to work to cultivate anti-tetanus serum under the aegis of SII, which he established in 1966. Agricultural land was bought and repurposed for the stud farm and vaccine factory, and scientists were poached from the Haffkine Institute, which was the first vaccine manufacturer in the subcontinent during the colonial period and later became a public sector undertaking. Lobbying for state protection for domestic capital and circumventing agrarian laws with the help of local authorities, the SII gradually scaled up business to produce multiple vaccines. The speculative business of horse breeding thus morphed over time into the extractive business of vaccine manufacturing.
Specifically, within the context of Covid-19, the centrality of SII has been aided by several factors. On the international stage an important development was its early invitation into the Oxford University-based Vaccitech Ltd. consortium and its eventual position as an important sub-licensee to AstraZeneca. On the domestic front, on April 20, 2021, the SII received $400 million from the Indian central government’s vaccination budget to ramp up mass production of the Oxford-AstraZeneca vaccine. (Concurrently, Bharat Biotech received $200 million to ramp up production of the indigenously developed Covaxin). This funding, which amounts to 10% of the entire vaccine budget in 2021-22, was presented as an advance payment for vaccines that the SII was supposed to produce and supply in the next 2-3 months. Notably, this funding was advanced to SII and Bharat Biotech without a bank guarantee or collateral, as an exception to Rule 172 of the government’s General Financial Rules. Similar levels of non-transparency around the budget allocation for healthcare and the non-availability in the public domain of the contract between the Indian state and SII suggest mis- or dis-information circulating around the extent to which public monies are implicated in vaccine profits.
The Indian state’s approach to securing vaccines thus follows the classic (and global) incentive and subsidy approach for vaccine manufacturers: a demand guarantee and a price floor. In the name of mitigating risks for innovation, this approach has funneled public money into two private sectors, vaccine manufacturing and as we shall show now, through drug pricing into privatized health care.
Horse-racing, Speculation, Extraction, and Immiseration
Identifying the Global North-South divide as the central contradiction, and employing this identification as an argument against TRIPs, implies a certain diagnosis: in this story, the push for prolonged patent protection by states in the Global North fosters market monopoly, thus allowing drug companies to extract profits through marketing and pricing. Two major reasons are advanced against patent protection: firstly, the fact that lifting them does not affect the bottom line for big Pharma; and secondly, that corporations exaggerate the risks involved in vaccine production, since considerable public investment makes innovation possible in the first place. An argument against the patent regime is thus necessary, as Walden Bello has argued, for empowering developing countries.
But is patent protection the only thing standing in the way of people’s access to vaccination and 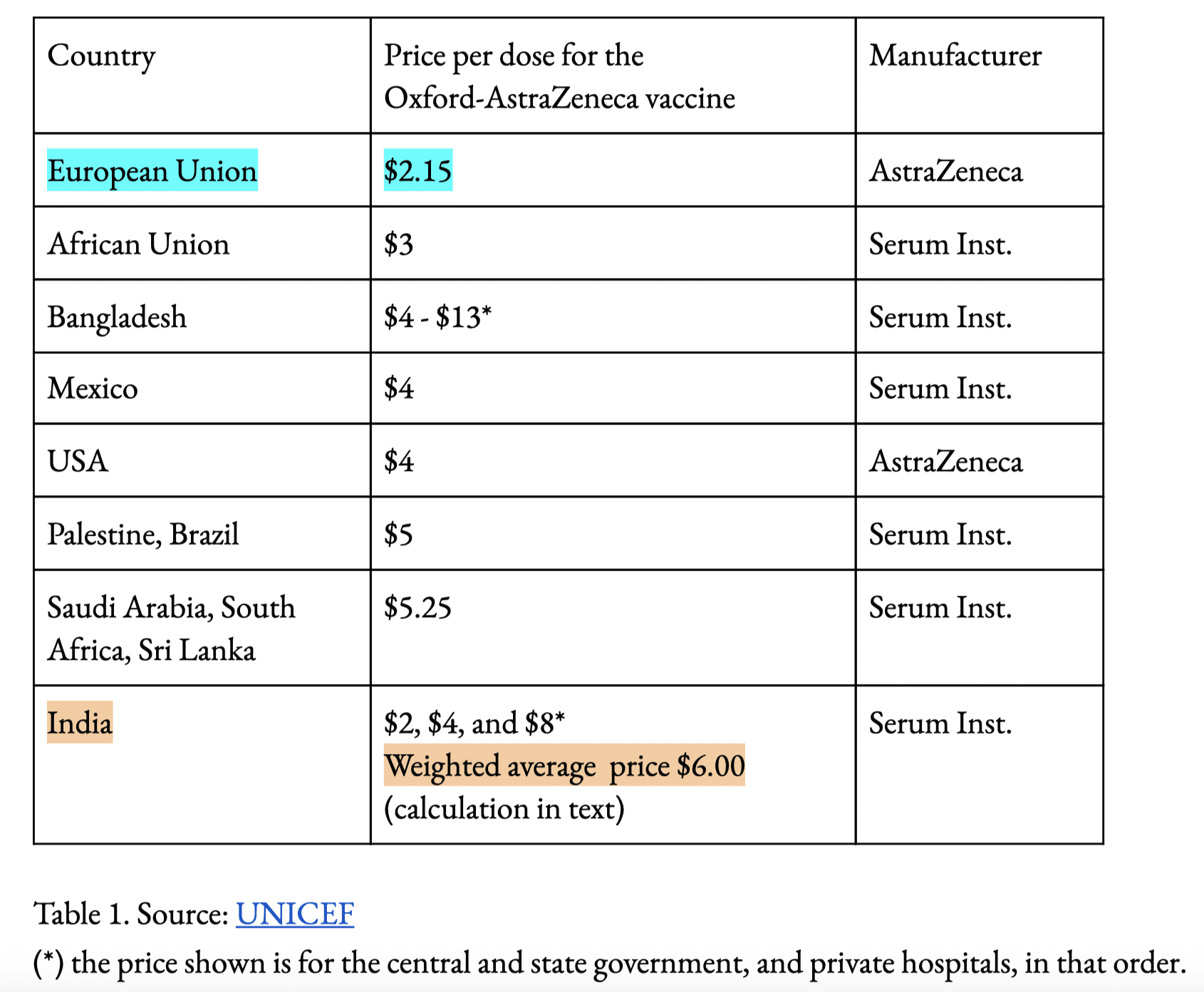 healthcare? Vaccine geoeconomics is multifaceted. To probe this further, one needs to question the three imaginings of Poonawalla described in the introduction: the nationalist, the internationalist, and the broadly left-wing, which largely leave uncontested the claim that SII is manufacturing the “people’s vaccine.” This claim should be critically examined, since one of the most obvious markers of extraction is vaccine pricing.
healthcare? Vaccine geoeconomics is multifaceted. To probe this further, one needs to question the three imaginings of Poonawalla described in the introduction: the nationalist, the internationalist, and the broadly left-wing, which largely leave uncontested the claim that SII is manufacturing the “people’s vaccine.” This claim should be critically examined, since one of the most obvious markers of extraction is vaccine pricing.
The SII, which manufactures and distributes the Oxford-AstraZeneca vaccine under the name Covishield, is charging $2.03 per dose for the Indian central government, $4.06 per dose for Indian state governments, and $8.12 per dose for the Indian private market. Bharat Biotech, which distributes the domestically made Covaxin, is charging the same amount per dose for the central government and double for state governments and private hospitals. It is instructive to compare these prices to what the SII is charging other countries, as well as the price AstraZeneca is charging the European Union and the US. This is available from UNICEF data, shown in the accompanying table.
It is clear that the price being paid per dose by state governments in India to the SII far exceeds that being paid by the EU to AstraZeneca. The price for private hospitals in India is even higher and there have been suggestions that the Modi government will push the entire 18-45 year old population into the private vaccine market. Given that around 30% of the population is below 15 years old and hence ineligible for the vaccine, 65% are in the age group 15-64, and only 5% are older, one can roughly estimate that two-thirds of the vaccine-eligible population may finally be forced to buy the vaccine in the private market. (And this is a conservative estimate; the number might actually be higher, given that the median age is 27 years.) This gives a weighted price of the vaccine of around $6 per dose, or almost thrice that of the European Union. By the same calculation, Bharat Biotech’s vaccine comes to $12 per dose, or almost six times that of the European Union, albeit for a different vaccine. If one were to factor in the purchasing power parity, GDP per capita, or other obvious measures of disparity between India and the EU, the price differential becomes even starker. From the UNICEF data, it is clear that elsewhere – in Bangladesh, Sri Lanka, or the African Union – the pricing imposed by the SII is as steep or worse.
India’s working poor – the vast majority of the country – cannot afford the price tag for the two doses of Covishield or Covaxin. Given that the price of a Serum Institute vaccine is far beyond the reach of the vast majority of Indians, and much more expensive than those sold by the company to Europeans or Americans, it is clear that mass vaccination is not the priority of the Modi regime in India. The science is very explicit: unless the pandemic is controlled for a vast share of the population, it is going to continue. This two-tiered vaccination program, along with a largely digital vaccination registration drive and the deliberate miscalculation of the needs of the population, have thus served to create what can only be called a vaccine famine. India’s extensive domestic infrastructure for vaccine dissemination and history of public sector vaccine companies, when juxtaposed with its current failure to vaccinate people, raises alarming questions about the future. Indeed, the fact that these policies continue to be pursued in the face of the alarming death toll suggests there may be no future for many people to prepare for at all.
The business press has by and large defended SII and Bharat Biotech, stating that the profit is required to invest in new capacity and faulting the government for not investing early on. Comparisons to India’s successful vaccination against polio and pox have been called “specious” by the Hindu Business. The Economic Times claims that the Serum Institute’s $2 price per dose (the rate for the central government) “does not leave it with any surplus for investing in new capacity.” This can be contested on at least two grounds. Firstly, AstraZeneca is selling its vaccine at the same price to the European Union. Even if one accepts AstraZeneca’s contention that it is operating on a non-profit basis (a contention that has not been verified), it should be kept in mind, as we have seen, that the weighted average price for India actually comes to around $6.
Poonawalla’s company is raking in immense profits. In fact, the Serum Institute is expected to generate $1 billion in profits from the Covid vaccine by 2021, with projected profits of $4 billion by 2022. It is a highly profitable company according to data from India’s Ministry of Corporate Affairs, with annual revenues and profits around $800 million and $300 million respectively for 2020. Covid has been particularly lucrative for vaccine companies in general. According to a People’s Vaccine Alliance report, the improving fortunes of SII along with other vaccine companies has produced new billionaires. During this period, Poonawalla Finance has diversified and acquired several holdings, including the Wellness pharmacy chain, portending potential vertical integration in the pharmaceutical industry in India.
What is the endgame of vaccine capitalism? What kind of future does the might of India’s pharmaceutical industry and the extraction and immiseration perpetrated by the state and vaccine capital portend? The inexorable future toward which vaccine capitalism is taking us is a Covid endemic: a future where Covid is a treatable disease for the upper middle classes and a continuous deadly infectious disease with a steady level of fatalities among the poor. Post-pandemic vaccine pricing and royalty flows almost guarantee an indefinite and infinite future demand for vaccines, which will be priced at far above their current rates and will, on the one hand, serve as a conduit through which massive wealth will be transferred from the public to the private sector, while on the other, being used by the Indian state as soft power currency and foreign policy cudgel.
We see the same problem of risk mitigation and the bifurcation of distribution through differential pricing on a global scale via GAVI. It is important to examine how appeals for vaccine security in the current conjuncture have also been perverted for competition over trading blocs, a topic to which we turn next.
Beyond the North-South Duality: The Making of a Vaccine Famine
The appeal of frameworks like “vaccine imperialism” lies in their coherence: a coherence that allows one to stake out mutually opposed political positions. Yet the geopolitics of vaccine has played out over a complex terrain of patents, multilateral purchase agreements, public-private partnerships, and financial bonds. Over the course of 2020-21, as new vaccine candidates started emerging before clinical trials were underway, trade agreements over testing and bulk manufacturing began shifting dynamically.
A publication of the Council on Foreign Affairs notes, of the BRIC countries, three (Russia, India, and China) “have taken a global approach to vaccine diplomacy—i.e., providing vaccines to at least ten countries on three continents or more…in alignment with their national and strategic interests.” In May 2020, China’s President Xi Jinping pledged to make the country’s Covid-19 vaccines a “global public good.” As China began to set up its cold chain vaccine air bridge to Ethiopia, various Chinese companies began to sign agreements for supplying vaccines to Brazil, Turkey, Mexico, or testing or co-manufacturingwith countries like Morocco. By November 2020, Russian Direct Investment Fund (RDIF) signed a deal with the Moroccan manufacturer Galencia to produce Sputnik locally. In early March 2021, the Quad Vaccine Partnership between Australia, Japan, India, and the United States was announced, which promised to deliver a billion extra doses by the end of 2022. The Quad is being presented as a counterweight to Chinese and Russian dominance over the vaccine market.
The Serum Institute of India is the main production site for both COVAX and Quad commitment. According to the Ministry of External Affairs of the Government of India, vaccines made in India by the SII are being supplied to over 95 countries, including the traditional spheres of influence in South and Southeast Asia, but also across vast swathes of Africa under the aegis of the COVAX project.
On the color-coded global vaccine map that displays nation-states in varying shades of red and yellow, depending on the extent to which they have been (and will be) left behind by the vaccine scramble, we can superpose another color-coded map of the world as multiple trading blocs. This is reminiscent of the Scramble for Africa and the contest over trading blocs in the post-World War II era. Given that less than 1% of vaccines are manufactured within the African continent, and 70% of the supply of vaccines comes by way of Indian players (chiefly SII) via GAVI, the African CDC recently emphasized a policy approach that further connects vaccine security with manufacturing sovereignty. In a move that is being called a vaccine revolution, the 10 identified manufactures are consolidated in 5 countries with Johnson & Johnson and the South African manufacturing pharmaceutical giant Aspen Pharmacare entering into bulk manufacturing agreements. Africa is the largest growing market for vaccines, with a potential to increase up to 2.3 to 5.4 billion dollars by 2030.
 But does the language of geopolitics alone really capture the current reality? Geopolitics has a tendency to color-code the world into manufacturing and recipient countries; the question of peoples’ vaccination then becomes translated into interstate distances in capital and diplomatic relations. Visuals such as the one shown here have a powerful impact on how we perceive the battlegrounds of politics; they are symptomatic of the lingering (but continually questioned) persistence of the geopolitical view that divides the globe into binaries like North and South; developing and developed; haves and have nots; good and evil. Crudely speaking, they carry state-centric understandings of global trade.
But does the language of geopolitics alone really capture the current reality? Geopolitics has a tendency to color-code the world into manufacturing and recipient countries; the question of peoples’ vaccination then becomes translated into interstate distances in capital and diplomatic relations. Visuals such as the one shown here have a powerful impact on how we perceive the battlegrounds of politics; they are symptomatic of the lingering (but continually questioned) persistence of the geopolitical view that divides the globe into binaries like North and South; developing and developed; haves and have nots; good and evil. Crudely speaking, they carry state-centric understandings of global trade.
Diffuse Capital, Porous Virus: Vaccine Bonds, GAVI, and Big Bucks
Operating within the theoretical framework of geopolitics and vaccine diplomacy obscures the dominant role played by capital, untethered from the state to varying degrees, in vaccine production, manufacture, and distribution. Studying the case of the Oxford-AstraZeneca vaccine in this context is instructive: how does publicly funded research ultimately get into the hands of millions of people?
A paper appositely titled “How the ‘Oxford’ Covid-19 Vaccine Became the ‘AstraZeneca’ Covid-19 Vaccine” published in Medicines Law and Policy shows the interstitial bonds that exist among universities, pharmaceutical companies, and venture capital at all stages of development and production of the AstraZeneca vaccine. Researchers at the Jenner Institute at Oxford University first developed the viral vector technology that underlies the AstraZeneca vaccine; they then founded a spin-out company called Vaccitech Ltd. in 2016 to further develop this technology. The minority stakeholders of Vaccitech Ltd. are a combination of Oxford University and individual researchers; the majority is a web of venture capitalist firms with the biggest one being OSI, an umbrella of further companies like Tencent, Google Ventures, and Sequoia Heritage, as well as charitable foundations like the Wellcome Trust. Vaccitech Ltd. entered into an exclusive agreement (engineered by Bill Gates) with AstraZeneca in April 2020, for the “international distribution of the vaccine, particularly working to make it available and accessible to low and medium income countries.” AstraZeneca subsequently entered into sub-licenses with several companies in the US, Europe, and Asia – notably the Serum Institute of India.
The authors would like to thank Kasturi Basu and Srinivas Lankala for insights that improved our understanding. We would also like to thank Atreyi Dasgupta and Rohini Hensman for a careful reading of the draft, and Orijit Sen for use of his artwork.

This labyrinthine network of venture capital and pharmaceutical companies that is embedded at every stage of the Oxford-AstraZeneca vaccine all stands to profit from current and post-pandemic royalties. As profits flow back from sub-licensees like the Serum Institute to the main licensee AstraZeneca to the venture capital that constitutes Vaccitech Ltd., it raises deep questions about the nature of capital extraction, states, and their inter-relation.
Even international structures which appear to be guided by the state-centric framework of geopolitics, reveal, on deeper investigation, to be undergirded by networks of tethered and untethered capital. Thefunding mechanism of GAVI, the Vaccine Alliance, demonstrates this vividly. Launched in 2000, GAVI brings together the WHO, UNICEF, the World Bank, the Gates Foundation, and representatives of governments with the aim to finance vaccine programs in low-income countries. Donor governments make multi-year pledges; these pledges are converted to immediately available funds for GAVI by issuing vaccine bonds in capital markets, where investors buying these bonds are repaid with interest. The vehicle that issues these bonds is the International Finance Facility for Immunisation (IFFIm). Bonds are purchased from IFFIm in the market by asset managers, pension funds, insurance funds, banks, and corporations at typical semi-annual coupon rates of 0.375%.
Thus, not only do vaccine bonds provide a lucrative source for investors to diversify their portfolios and get attractive, low-risk returns, but this can be conducted under the veneer of social responsibility. Indeed, Cyrus Ardalan, IFFIm Board Chair, stridently declares, “A child not immunized today may be a life lost tomorrow. Let’s invest in life now.” In the language of vaccine bonds, investing in life amounts to a coupon rate assessment. The GAVI-IFFIm entity is not the only player in the vaccine bond market. The African Development Bank, the World Bank’s International Finance Corporation and other entities all issued bonds in 2020, at levels that are 12 times higher than 2019 investments. The pandemic is big bucks; the bond markets are abuzz with activity. The prospect of vaccinating 3.5 billion people is likely to energize this market further. In April 2021, the IFFIm issued $750 million 5-year vaccine bonds at a semi-annual coupon rate of 1%.
From university-based research to scaled-up manufacturing to the final jab in the arm, the mechanics of vaccines is determined by a complex interlocking network of capital – some nominally tethered to the structure of the state through manufacturing licenses, labor, or location; others untethered, like venture capital that invests in Vaccitech Ltd. or that buys IFFIm bonds. Visualizing this mechanics as a triad of developing, industrialized, and donor countries participating in GAVI; or a dyad of Big Pharma like AstraZeneca and sub-licensees like the Serum Institute performing scaled-up manufacturing obscures this reality.
The neatly divided geopolitical language of the Global North and Global South is eroded by the diffused geography of pandemic capitalism and the virus itself. One of the most macabre features of pandemic capitalism is the way in which the biological overlaps with the political. The virus SARS-CoV-2, which causes the Covid-19 illness, is essentially a simple set of instructions encoded on a chemical called RNA, wrapped in a coat made of protein. The virus relies on other cells to replicate itself and, when unchecked, it mutates as it spreads, gaining virulence. Pandemic capital, too, is both tethered to the infrastructure of the state, to the geopolitical social and the body politic of nations; but like the virus it transcends the boundaries of nations. The second wave of Covid in India has once again revealed the global supply chains that undergird vaccine manufacture and the porous boundaries of nation states – made so by the movement of materials, people, viruses, bonds, risks, investments.
Conclusion
The CFO of Pfizer, Frank D’Amelio, offers a quantitative outlook for post-pandemic profit flows:
[D]uring an earnings call in early February, Pfizer CFO Frank D’Amelio described Pfizer’s $19.50-per-dose price as “pandemic pricing” and “that’s not a normal price like we typically get for a vaccine, $150, $175 per dose.” D’Amelio said just a bit later during the call, “Now let’s go beyond a pandemic-pricing environment, the environment we’re currently in. Obviously, we’re going to get more on price. And clearly, to your point, the more volume we put through our factories, the lower unit cost will become. So clearly, there’s a significant opportunity for those margins to improve once we get beyond the pandemic environment that we’re in.” Like Pfizer, Moderna has indicated that it may raise its prices after the pandemic ends, anticipating that COVID-19 will be endemic. The Moderna CEO said during a conference call last year that the pandemic pricing would be “well below value.”
Whither vaccine imperialism then? What of the language of vaccine diplomacy, geopolitics, and the Global North versus the Global South? Remaining ensconced within the broader ambit of capital, this language, often emanating from the Left and ostensibly directed against the West, has little power to confront immiseration in a post-pandemic future. Unless firmly opposed to vaccine capitalism – the commodification of public health and medicine, the loot of public wealth – unless militantly poised against the enormous power of venture capital and vaccine corporations, from AstraZeneca to SII, such a framework ultimately amounts to taking sides with one form of capital versus another.