
To be sure, there are many other disabled people who have simply fallen through the cracks, so to speak, in the decades and years since deinstitutionalization and the onset of the neoliberal shredding of the social safety net. Some – especially those with various psychological impairments – have ended up living on the street or in transient settings, often unsafe, precarious, and isolating. Many become entangled in various alternative systems of institutionalized control, abuse, and carcerality. The Center for Disease Control reports that between 1992 and 2003, the number of people with psychological impairments or disabilities visiting emergency rooms nationwide increased by 56 percent, from 2,381,000 to 3,718,000.28As cited in Rembis, “The New Asylums,” sec. Why So Many Mad Prisoners?, para. 5. Understaffed and underfunded, many emergency rooms often turn these people back out onto the street without providing either adequate treatment or support. The result is a situation that funnels disabled people into the extensive grasp of the sprawling U.S. system of mass criminal incarceration.
The Era of Mass Incarceration
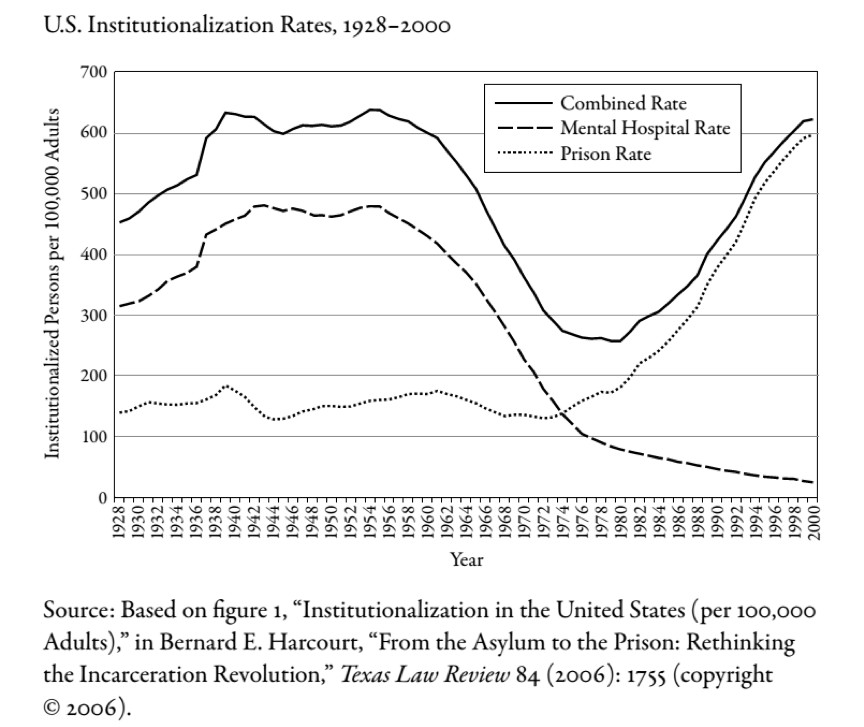
At the precise moment that deinstitutionalization was bringing one era to a close, a different era of institutionalization was just kicking off in the U.S. Referred to as “mass incarceration”, it has been characterized by the unprecedented and precipitous expansion of the nation’s state and federal system of criminal prisons and jails.29Michelle Alexander, The New Jim Crow: Mass Incarceration in the Age of Colorblindness, eBook (New York: New Press, 2012). As Figure 1 demonstrates, the rate of prison incarceration in the U.S. began to explode just as the rate of institutionalization was approaching its nadir.
Figure 130As reproduced in Parsons, From Asylum to Prison, 11.
By the first decade of the twenty-first century, the U.S. incarcerated a greater share of its population than any other country; a rate of one per one hundred adults, or 2.28 million people.31Ben-Moshe, Chapman, and Carey, “Reconsidering Confinement,” sec. Resistance, Reform, and Reiteration, para. 7. If all those under some form of supervision or control by the criminal-carceral system are included (i.e., prison, jail, probation, parole), then the population is closer to seven million, or one in every thirty-one residents. As with everything in the U.S., mass incarceration is structured, too, by systems of racial and gender inequity. Black men are 6.5 times more likely than white men to be imprisoned; Black women are 3 times more likely than white women to be imprisoned.32Rembis, “The New Asylums,” sec. Counting Mad Prisoners, para. 1.
Though not causally connected, the roughly sequential phenomena of deinstitutionalization and mass incarceration are related in significant material respects. Many states utilized the direct budgetary savings accrued from the closure of institutions in order to fund the construction of prisons. More directly, the very lands and buildings that formerly housed state institutions were often immediately repurposed and reopened as prisons.33Nirmala Erevelles, “Crippin’ Jim Crow: Disability, Dis-Location, and the School-to-Prison Pipeline,” in Ben-Moshe, Chapman, and Carey, Disability Incarcerated, sec. “Coming Out Crip” in Incarcerated Spaces, para. 1; Parsons, From Asylum to Prison, 9.In facilities across upstate New York, the process of deinstitutionalization was actually accelerated by the desire of state officials to obtain expanded prison space.34Castellani, From Snake Pits to Cash Cows, 242.
Today, disabled people have come to account for a disproportionate segment of the incarcerated population.35Parsons, From Asylum to Prison, 4–5.This includes a particular over-representation of people with psychological impairments. A 2006 report from the Bureau of Justice Statistics put the number of jail inmates who “have a mental health problem” at 64% of the total, the number of federal inmates at 45%, and the number of state prisoners at 56%.36As cited in Rembis, “The New Asylums,” sec. Counting Mad Prisoners, para. 2. There are several reasons for this.
- Mass incarceration has led to an absolute increase in the total number of people in prisons and jails, which includes a constituent increase in the number of people with psychiatric disabilities who have been caught in the net of the criminal legal system.37Parsons, From Asylum to Prison, 5.
- Disabled people tend to disproportionately be poor, homeless, and vulnerable. For this reason they tend to disproportionately experience far greater points of contact with police and other carceral state forces and agencies.
- As part of the prison boom, and occurring contemporaneous to deinstitutionalization, former disabled institutional residents as well as those who had remained in the community, along with the newly disabled, found themselves increasingly persecuted by changes in the law. Disability Studies scholar Michael Rembis explains, “[L]awmakers, business owners, neighborhood residents, and some family members began fashioning local, state, and federal policies and programs designed primarily to segregate, isolate, and in many cases criminalize behaviors that in earlier decades or other settings may not have warranted legal or juridical intervention.”38Rembis, “The New Asylums,” sec. The (Hi)stories We Tell, para. 2.
- Poverty and prison, two intimately connected systems of oppression, are both eminently injurious and disabling. The experiences of imprisonment itself including internal regimes of punishment and confinement, isolation from social contact with family, friends, and communities, the self-alienation inherent to carceral dehumanization, and the constant (re)traumatization are all incredibly generative of mental illness and psychological debilitation. The same goes for the production of physiological impairments, which are rife in carceral spaces. They are produced or deepened by unsafe and unregulated working conditions, unhealthy quality of air, food, and sanitation, violence and sexual assault, and poor or non-existent access to and standards of medical care, especially vis-à-vis the spread of infectious diseases.39Stewart and Russell, “Disablement, Prison, and Historical Segregation.”
Theories of Disability Incarceration
There are different ways to think about the intersection of various forms of social oppression and prison through an abolitionist framework. Viewed through a lens of racialized capitalism and the history of the caste-like exploitation and oppression of Black people in the U.S., the present era of mass incarceration and expanded criminalization can be likened to a novel, de facto “Jim Crow”, the colloquial name for the de jure matrix of racial segregation and domination that prevailed after the end of Reconstruction.40Cf., Alexander, The New Jim Crow; Ruth Wilson Gilmore, Golden Gulag: Prisons, Surplus, Crisis, and Opposition in Globalizing California (Berkeley: University of California Press, 2007); Ruth Wilson Gilmore, Change Everything: Racial Capitalism and the Case for Abolition (Chicago: Haymarket Books, 2020).Mass incarceration can also be understood as a function of political economy with respect to the control of “surplus populations.” This refers to those who are rendered redundant or unassimilable by the prevailing conditions of capitalist production (and distribution), and who are thereby effectively cut off from routes to social integration.
Surplus population theory can be used to explain the disproportionately high rates of impoverishment, unemployment, and imprisonment of a number of historically oppressed social groups, including Black and disabled Americans.41Charlton, Nothing about Us without Us, 24; Stewart and Russell, “Disablement, Prison, and Historical Segregation”; Russell, Capitalism & Disability; Loïc Wacquant, Punishing the Poor: The Neoliberal Government of Social Insecurity (Durham, N.C.: Duke Univ. Press, 2009), 207; Erevelles, “Crippin’ Jim Crow,” sec. Compulsory Able-Bodiedness in the Postcolonial Ghetto, para. 3.However, it is important to clarify that such groups are considered “surplus” or “superfluous” people from the standpoint of capital. In absolute terms, there exists more than enough wealth and resources to be comfortably shared by all humans, and all humans in turn have the unique capacity to contribute in some integral form to the general wealth of collective human experience.
Another view worth considering is what might be termed critical behaviorism. This view holds that there are deep connections between the neoliberal elimination of the social-welfare safety net and the rise of mass incarceration. It describes a new paradigm jointly pathologizing, criminalizing, and persecuting an array of behaviors, mind states, and medically-diagnosed psychological phenomena, collectively referred to as “madness.”42Rembis, “The New Asylums.” This process has been both politically-motivated and racially-driven, and has been attended by the vast expansion of the psychiatric-industrial complex.
For instance, starting in the 1960s schizophrenia morphed from a disease disproportionately assigned to White women into one disproportionately assigned to Black men, simultaneously taking on an association with violent social behavior.43Jonathan M. Metzl, The Protest Psychosis: How Schizophrenia Became a Black Disease, eBook (Boston: Beacon Press, 2009); Rembis, “The New Asylums,” sec. Counting Mad Prisoners, para. 4.In The Protest Psychosis: How Schizophrenia Became a Black Disease, author Jonathan Metzl reviews articles and studies published in psychiatric journals between the 1970s and 1990s, which revealed that Black patients were up to seven times more likely than White patients to be diagnosed with schizophrenia, and far less likely than White people to be diagnosed with mental illnesses such as depression.44Metzl, The Protest Psychosis, Preface, para. 6. Metzl notes that there is in fact a long history in the U.S. of psychiatric diagnosis being used in the service of racism. In the 1850s, Black slaves who frequently ran away from their masters were said to be afflicted by a mental illness called drapetomania. Slaves who exhibited unruly behavior and disrespect for the master’s property were said to have dysaesthesia aethiopis, a condition advisedly ‘cured’ by extensive whipping. Metzl, Preface, para. 2.
This argument strongly undercuts a particularly specious and reactionary thesis advanced in the wake of deinstitutionalization. Whereas one side accuses the system of mass incarceration of exposing entirely new swathes of the population to the reach of institutional carcerality, the other proposes a direct causal link between deinstitutionalization and mass incarceration. A number of articles written in the 1980s and 1990s, including one published as recently as 2015 in the Journal of the American Medical Association, argued that deinstitutionalization went too far and that the closure of mental hospitals led to the dramatic rise in homelessness and incarceration. What is needed now, they argue, is stricter involuntary treatment laws and a return to the institutional asylum model of yesteryear.45E. Fuller Torrey, Nowhere to Go: The Tragic Odyssey of the Homeless Mentally Ill (New York: Harper and Row, 1988); E. Fuller Torrey, Out of the Shadows: Confronting America’s Mental Illness Crisis (New York: Wiley, 1998), 193-203; Ben-Moshe, Chapman, and Carey, “Reconsidering Confinement,” sec. Interlocking Analysis and Particularity, para. 4; Dominic A. Sisti, Andrea G. Segal, and Ezekiel J. Emanuel, “Improving Long-Term Psychiatric Care: Bring Back the Asylum,” Journal of the American Medical Association 313 (January 2015): 243–44; Parsons, From Asylum to Prison, 3–4. This not only shifts the blame for capitalist economic inequality and repressive ruling class policy onto disabled people, it undermines the very notion that disabled people are capable of living autonomous lives free of carceral oppression.